
Intrusive Thoughts: Why the Mind Gets Stuck on Unwanted Ideas

Many people have had the experience of a thought appearing suddenly while doing something completely ordinary like driving, washing dishes, or sitting in a meeting. The thought can feel disturbing, confusing, or completely out of character, and the first reaction is often a moment of surprise. Why did my mind just go there? A person might briefly imagine swerving their car into traffic, saying something inappropriate out loud, or picturing something bad happening to someone they care about.
For some people, the thought passes quickly and is forgotten. For others, the mind latches onto it and begins turning it over repeatedly. The more a person tries to push the thought away, the more persistent it can become. This is the part most people are never taught. Trying harder to eliminate the thought often increases how strongly it sticks.
Intrusive thoughts are unwanted thoughts or mental images that appear without warning and usually conflict sharply with a person's values and sense of self. They are not plans. They are not desires. They are not evidence of hidden intent. They are extremely common, but when the mind becomes stuck on them, the experience can feel confusing, isolating, and difficult to talk about.
For individuals across Alberta, virtual counselling can help people better understand why intrusive thoughts happen and how to respond to them in a way that reduces their intensity over time.
Table of Contents
- What Are Intrusive Thoughts?
- Why Intrusive Thoughts Feel So Disturbing
- Common Types of Intrusive Thoughts
- Why the Mind Gets Stuck on Certain Intrusive Thoughts
- Intrusive Thoughts in Anxiety, OCD, and Trauma
- Evidence-Based Therapy for Intrusive Thoughts
- How to Respond to Intrusive Thoughts: 3 Practical Strategies
- Therapy for Intrusive Thoughts in Alberta
- Frequently Asked Questions About Intrusive Thoughts
What Are Intrusive Thoughts?
Intrusive thoughts are unwanted thoughts or images that appear without intention and feel sharply at odds with what a person actually wants or values. They are not a sign of hidden desire. The clinical term for this conflict between a thought and a person's sense of self is ego-dystonic, which simply means the thought feels foreign, not like you. That distinction matters more than most people realize.
Intrusive Thoughts Are Unwanted Thoughts, Not Intentions
One of the most important things research has clarified is that the content of an intrusive thought says nothing reliable about a person's character or intentions. Stanley Rachman and Padmal de Silva's foundational research in the late 1970s found that the vast majority of people without any mental health diagnosis experience intrusive thoughts with content nearly identical to what clinicians see in OCD. Thoughts about violence, sex, contamination, and harm are not rare aberrations. They are part of how the human mind generates content, most of which passes through without notice.
What separates a thought that passes from one that sticks isn't the content. It's the meaning a person assigns to it.
Why Almost Everyone Experiences Intrusive Thoughts
The brain produces thousands of thoughts every day, and not all of them are rational, flattering, or consistent with who we are. That's not a flaw in the system. It's what a pattern-generating organ does. The mind is constantly running through possibilities, including ones that are unpleasant or disturbing. For most people, these pass quickly without comment. For others, usually because of anxiety, stress, past trauma, or how the thought gets interpreted, the thought catches and begins to loop.
Examples of Intrusive Thoughts People Rarely Talk About
People rarely describe their intrusive thoughts to anyone because the content feels too strange or too shameful. Some common examples: imagining pushing someone in front of a car while standing at a crosswalk, having a sexual thought about someone completely inappropriate, suddenly wondering whether you actually love your partner, fearing you said something offensive with no memory of doing so, or picturing something terrible happening to someone you care about. These examples are uncomfortable to read. They're also experienced by people who are caring, responsible, and mentally well.
Why Intrusive Thoughts Feel So Disturbing
When Thoughts Conflict with Personal Values
Intrusive thoughts tend to be most distressing when they target what a person cares about most. A devoted parent imagines harming their child. A religious person has a blasphemous thought mid-prayer. A gentle person imagines something violent. The distress is proportional to the conflict between the thought and the person's values, which is exactly why that distress is not a warning signal. It's evidence of the opposite. People who don't care about something don't suffer when they think about it.
Why the Brain Treats Intrusive Thoughts as Threats
There's a cognitive pattern called thought-action fusion. In plain language, it's the mistaken belief that having a thought makes it more likely to happen, or that thinking something is morally the same as wanting it. When this pattern is active, the brain treats the intrusive thought as a genuine threat rather than a passing mental event. Anxiety activates. Attention narrows. The thought, now flagged as dangerous, becomes harder to dismiss. This is the mechanism driving most of the distress, not the thought itself. Understanding how anxiety works can help make sense of why this loop escalates the way it does.
Why Trying to Push Thoughts Away Often Makes Them Stronger
Daniel Wegner's research demonstrated something counterintuitive: when people try to suppress a specific thought, they often think about it more. The classic experiment asked participants not to think about a white bear. Most couldn't stop. The reason is straightforward. Suppressing a thought requires the brain to keep checking whether the thought is gone, and that monitoring process keeps the thought active. Every time the mind checks, it finds the thought. The very act of trying not to think about something becomes the thing that keeps it present.
How Shame Keeps People Stuck in Silence
Most people with intrusive thoughts don't tell anyone about them. The content feels too frightening or too embarrassing, and the fear of being misunderstood is real. So the thoughts stay private, which means the person never learns that what they're experiencing is common, well-understood, and treatable. That silence tends to make the shame heavier, and heavier shame makes the suppression cycle harder to step out of. For many people, the weight of that isolation compounds existing stress and keeps the pattern running longer than it needs to.
Common Types of Intrusive Thoughts
Intrusive thoughts are not one uniform experience. The content varies widely, and readers need to find their specific situation here, because the type of intrusive thought often shapes how a person responds and how distress shows up.
Harm-Related Intrusive Thoughts
These involve fear of hurting someone else or, less commonly, oneself. A person might imagine stabbing a family member while cooking, pushing a stranger, or losing control of their car. These are different from suicidal ideation, which involves a desire or plan; harm-related intrusive thoughts are characterized by horror at the thought, not attraction to it. They appear across anxiety presentations and are not exclusive to OCD.
Sexual Intrusive Thoughts
Unwanted sexual thoughts or images that conflict sharply with a person's values or identity. This might involve taboo scenarios, inappropriate partners, or content that feels deeply inconsistent with how the person sees themselves. The distress is the indicator that the thought is unwanted, not a reflection of hidden desire.
Religious and Moral Intrusive Thoughts
Sometimes called scrupulosity, this presentation involves blasphemous thoughts, fear of having sinned, or an overwhelming sense of moral contamination. A person might experience intrusive images during prayer or worship, or feel that certain thoughts have spiritually compromised them. This is one of the less-discussed presentations in mainstream mental health content, but it's well-represented in clinical OCD and anxiety literature.
Relationship Doubt and Fear-Based Thoughts
Relationship OCD, sometimes abbreviated as ROCD, involves obsessive doubt about a romantic relationship. Does my partner really love me? Do I actually love them? Is this the right relationship? These thoughts feel urgent and convincing, and they differ from normal relationship ambivalence in their persistence and the level of distress they generate. They tend to be accompanied by compulsive reassurance-seeking or mental reviewing that provides temporary relief but maintains the cycle. This pattern often shows up alongside broader difficulties with emotional regulation.
Health Anxiety and Intrusive Thoughts
Intrusive images or fears about illness, physical symptoms misread as signs of serious disease, or repeated mental reviewing of physical sensations. The intrusive element is the thought's involuntary return and the anxiety it carries, not the health concern itself. This presentation often overlaps with generalized anxiety and can look similar on the surface while operating slightly differently underneath.
Trauma-Related Intrusive Thoughts
Flashback imagery, intrusive sensory memories, or unwanted mental replays of traumatic events. These operate differently in the brain from OCD-type intrusive thoughts: they involve involuntary memory retrieval rather than interpretation-driven loops. Bessel van der Kolk's research on how trauma is stored in the body and nervous system helps explain why these intrusions can feel present-tense rather than like memories of something that already happened.
Why the Mind Gets Stuck on Certain Intrusive Thoughts
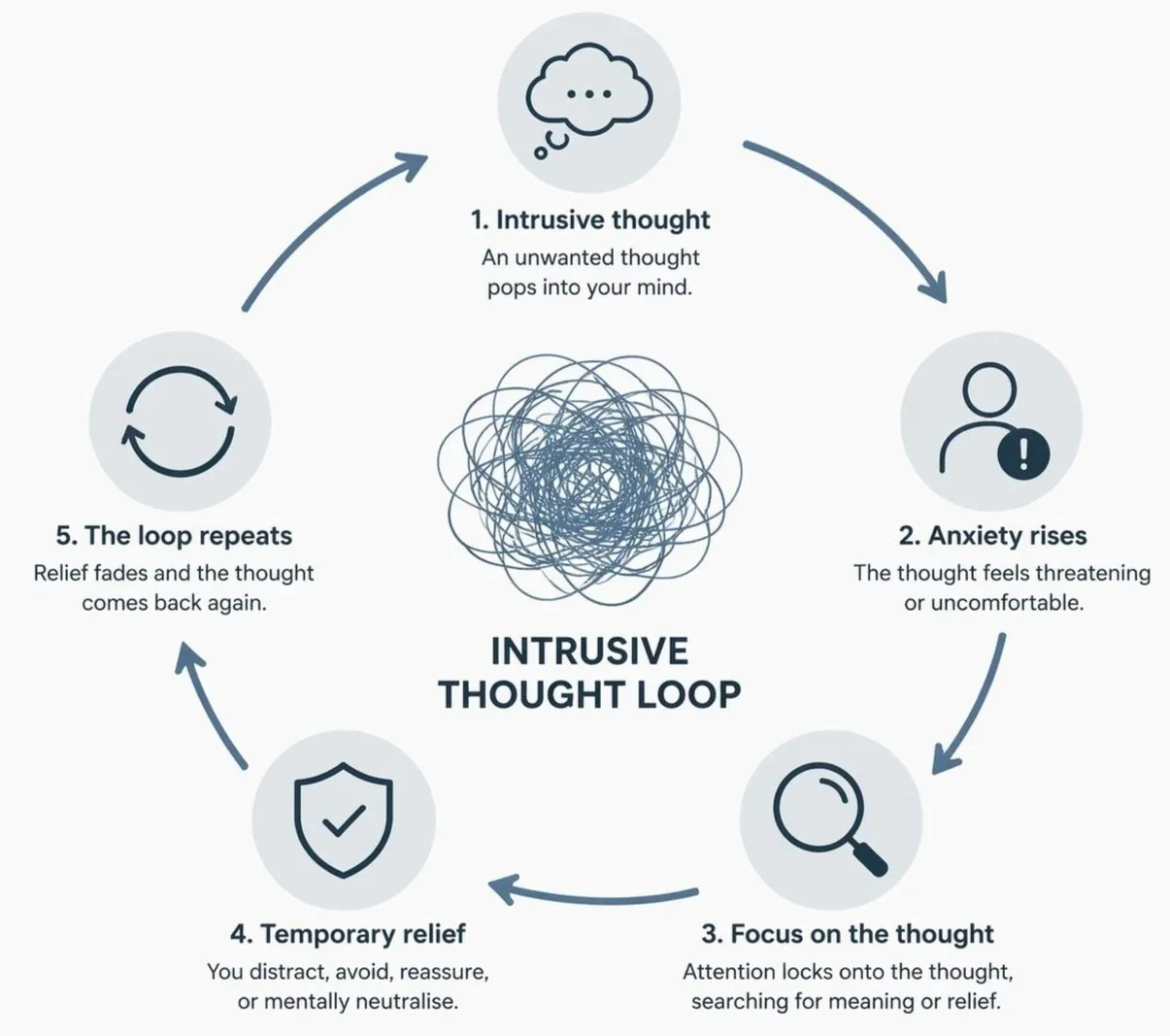
The Intrusive Thought Loop
Intrusive thoughts often persist because the brain gets pulled into a predictable cycle. The thought itself is not the main problem. What happens after the thought appears is what determines whether it passes quickly or becomes sticky.
The cycle often unfolds like this:
An unwanted thought appears suddenly
The thought feels important, alarming, or uncomfortable
Attention locks onto the thought, trying to understand what it means
The person tries to reduce the discomfort by analysing, avoiding, reassuring themselves, or mentally checking
Anxiety drops briefly, which creates a sense of relief
The brain learns that the thought required attention, so it flags it again later
Each time the cycle repeats, the thought can feel more significant and harder to ignore. This is not because the thought is dangerous, but because the brain has learned to treat it as something that needs monitoring. Most evidence-based therapies focus on helping people step out of this loop rather than trying to eliminate thoughts completely.
One Common Part of the Loop: Thought Suppression
One of the most common responses to an intrusive thought is to try to push it away. This reaction is completely understandable, but research shows it often has the opposite effect.
When a person tries not to think about something, the brain must keep checking whether the thought is gone. That monitoring process keeps the thought active in awareness. The more effort a person uses to force the thought out of mind, the more frequently the brain checks for it, which makes the thought easier to trigger again.
This is why thoughts often return more strongly after attempts to suppress them. The mind is not malfunctioning. It is doing exactly what it was asked to do: repeatedly checking whether the thought is still there.
How Attention Makes Intrusive Thoughts Feel More Important
When a person repeatedly returns to a thought, by reviewing it, analyzing it, or checking how they feel about it, the brain registers that thought as significant. Attention signals to the brain that something is important. The more attention a thought receives, the more the brain tags it as something worth monitoring. This is one reason why intrusive thoughts can escalate during periods when a person is trying hardest to resolve them.
Why Reassurance Can Accidentally Strengthen Intrusive Thoughts
Seeking reassurance, Googling symptoms, asking someone if a thought is normal, mentally reviewing whether the thought means something, provides short-term relief. The anxiety temporarily drops. But the relief itself teaches the brain that the thought was a real threat requiring a response. The next time the thought appears, the threat signal is slightly stronger, and the pull toward reassurance is slightly more urgent. Over time, the reassurance cycle maintains and often intensifies the distress.
The Role of Stress, Burnout, and Anxiety
When mental load is high, sleep is disrupted, or anxiety is elevated, the brain's ability to filter and make sense of thoughts in context is reduced. Intrusive thoughts that might pass unnoticed during a calm period become stickier and harder to dismiss. Burnout specifically reduces the mental bandwidth available for perspective-taking, making intrusive content feel more significant than it is. Stress doesn't cause intrusive thoughts, but it reliably makes them louder.
Intrusive Thoughts in Anxiety, OCD, and Trauma
Intrusive Thoughts in Anxiety Disorders
In generalized anxiety, intrusive thinking often takes the form of involuntary worry: future-oriented, repetitive, and difficult to interrupt. The content tends toward catastrophe, relationship concerns, health, and performance. The pattern differs slightly from OCD-type intrusions in that the thoughts are less ritualized but equally persistent. Anxiety amplifies how frequently intrusive content appears and how significant it feels, which is part of why the two experiences are so often intertwined.
Intrusive Thoughts in OCD
A common misunderstanding is that OCD is defined by its thought content. Clinically, OCD is defined by the response to the thought: the compulsion, the neutralizing behaviour, the avoidance. Two people can have identical intrusive thoughts; the one whose response includes compulsive checking, mental reviewing, or reassurance-seeking is more likely to be dealing with an OCD presentation. The thought alone doesn't tell us much. What follows the thought is where the clinical picture becomes clearer.
Trauma-Related Intrusive Memories and Images
Trauma-linked intrusive content operates differently from anxiety or OCD presentations. The brain stores traumatic memories differently from ordinary ones, which is why they can return as fragments, sensory impressions, or images that feel immediate rather than historical. Van der Kolk's research describes how trauma memories can bypass the brain's normal way of recognizing something is in the past, arriving without a clear signal that the event is already over. Therapy for trauma-related intrusions typically looks different from OCD or anxiety treatment, which is why accurate understanding of the presentation matters.
Evidence-Based Therapy for Intrusive Thoughts
CBT for Intrusive Thoughts
Cognitive Behavioural Therapy targets the interpretation process: what a person makes the thought mean. Rather than trying to eliminate the thought, CBT works to shift the belief that the thought is dangerous or revealing in the way the person fears. This changes the emotional response to the thought, which reduces its stickiness over time.
ACT for Intrusive Thoughts
Acceptance and Commitment Therapy, developed by Steven Hayes, uses a process called cognitive defusion: learning to observe a thought as a mental event rather than a fact or instruction. Instead of fighting the thought or accepting its content as true, a person learns to hold it differently. The thought can be present without directing behaviour or generating sustained distress.
ERP Therapy for Intrusive Thoughts
Exposure and Response Prevention is a specialized form of CBT that is considered the gold standard treatment for OCD-linked intrusive thoughts. The process involves deliberately encountering the triggering thought or situation without performing the usual compulsive response. Over repeated exposures, the brain learns that the thought does not require action, and the anxiety response diminishes. It's uncomfortable in the short term and consistently effective over time.
EMDR for Trauma-Related Intrusive Thoughts
Eye Movement Desensitization and Reprocessing is particularly relevant when intrusive thoughts are rooted in past traumatic experiences. EMDR supports the brain's natural processing of traumatic memory, reducing the emotional intensity attached to the intrusive content. It's not a fit for all presentations, but for trauma-linked intrusions specifically, the evidence is strong.
How to Respond to Intrusive Thoughts: 3 Practical Strategies
Noticing Thoughts Without Assigning Meaning (ACT-Based Cognitive Defusion)
This technique comes from Acceptance and Commitment Therapy and takes less than five minutes to practise.
When an intrusive thought appears, instead of trying to push it away or argue with it, try this: add the phrase "I notice I am having the thought that..." before it.
So instead of: I might hurt someone. The thought becomes: I notice I am having the thought that I might hurt someone.
This works because it creates a small but meaningful gap between you and the thought. The thought is still there, but it's now something you're observing rather than something you're inside of. In clinical practice, this reduces the emotional charge attached to the thought without requiring it to disappear. Suppression demands the thought leave. Defusion simply changes your relationship to it. That difference matters: you're no longer in a struggle with the thought, which means the brain stops registering it as a threat requiring a sustained response.
Neutral Acknowledgement Instead of Reassurance-Seeking (CFT-Informed)
When an intrusive thought arrives and the pull toward reassurance is strong, whether that's Googling, asking someone, or mentally reviewing whether the thought means something, try this instead.
Say, either aloud or internally: "My brain generated a thought. It doesn't require a verdict."
Then redirect attention to whatever you were doing before the thought arrived. Not with force. Just a return.
The clinical mechanism here draws from Compassion Focused Therapy, developed by Paul Gilbert. Reassurance temporarily reduces anxiety but signals to the brain that the thought warranted a threat response. Neutral acknowledgement does the opposite: it treats the thought as a neutral brain-generated event, which is accurate, and declines to confirm the threat signal. Over time, this reduces the emotional weight the thought carries. It's slower and less satisfying in the moment than reassurance, and that's the point. Reassurance feels good because it works briefly. Neutral acknowledgement works because it doesn't feed the cycle.
Attention Training to Interrupt Mental Monitoring (Metacognitive Approach)
This technique comes from Adrian Wells' metacognitive therapy and addresses one of the root mechanisms behind intrusive thought persistence: the internal self-monitoring that keeps thoughts salient.
Here's a short version you can try right now:
Sit somewhere reasonably quiet. Without closing your eyes, bring your attention to the sounds in the room. Pick one sound and hold it for a few seconds. Then expand your attention deliberately to include two or three sounds simultaneously. Then add a physical sensation: the weight of your body in the chair, the temperature of the air. Hold all of these at once for about two minutes.
What this does: it trains attention outward, away from internal scanning. Much of the distress attached to intrusive thoughts is maintained by the brain's internal monitoring process, constantly checking whether the thought is still there, what it means, how you feel about it. This technique interrupts that monitoring by redirecting attention externally. It doesn't suppress the thought. It just gives the monitoring system somewhere else to be. With practice, this becomes easier to access when the internal loop begins.
Therapy for Intrusive Thoughts in Alberta
Intrusive thoughts are distressing in proportion to how much they conflict with who a person actually is. That conflict is uncomfortable, but it's not a warning about character. It's information about values. The mind generates content that feels foreign and frightening, and the most common response, pushing harder against it, reliably makes things worse. That's not a personal failure. It's a predictable outcome of how suppression works in the brain.
The good news is that the mechanism driving intrusive thoughts is well understood, and the tools for interrupting it are specific and learnable. With the right approach, thoughts take up less mental space over time, and daily life becomes easier to be present in.
If intrusive thoughts are affecting your daily life, your confidence, or your ability to be present, therapy can help clarify what's driving the pattern and give you structured tools for responding differently. At The Mental Health Clinic, therapists work with intrusive thoughts using approaches like CBT, ACT, ERP, and EMDR, matched to the specific presentation. Virtual counselling is available across Alberta for teens, adults, couples, and families. Whether you're in Calgary, Edmonton, Red Deer, or somewhere more rural, support is available.
Frequently Asked Questions About Intrusive Thoughts
Why Do My Intrusive Thoughts Feel So Real and Personal?
Intrusive thoughts feel personal because they often target what you care most about. The more a thought conflicts with your identity or values, the more alarming it feels. That alarm is uncomfortable, but it's a sign the thought is foreign to who you are rather than a reflection of genuine desire or intention.
Do Intrusive Thoughts Mean Something is Wrong with Me?
Not in the way most people fear. Having intrusive thoughts is common across the general population. What matters clinically is not the presence of the thought but how much distress it causes and how a person responds to it. Distress about a thought is typically evidence that the thought conflicts with your values, not that it reveals something hidden.
Can Intrusive Thoughts Be a Sign of OCD?
Intrusive thoughts are commonly associated with obsessive-compulsive disorder (OCD), but having intrusive thoughts alone does not mean a person has OCD. The key distinction is how a person responds to the thought. OCD typically involves compulsive behaviours such as checking, reassurance-seeking, mental reviewing, avoidance, or attempts to neutralize the thought. Many people experience intrusive thoughts during periods of stress or anxiety without meeting criteria for OCD. A therapist can help determine whether the pattern reflects OCD, anxiety, trauma-related stress, or another presentation.
Can Intrusive Thoughts About Harming Someone Mean I Am Dangerous?
This is one of the most common fears people carry in silence, and the clinical answer is clear: the distress attached to a harm-related intrusive thought is itself evidence that the thought is unwanted. People who genuinely intend harm don't typically experience significant distress about it. The presence of horror, guilt, or fear in response to a thought is not a warning sign. It's the opposite.
Can Intrusive Thoughts Get Better Without Therapy?
For some people, understanding the mechanism behind intrusive thoughts, particularly how suppression backfires, produces meaningful relief on its own. Self-directed practice with defusion and attention techniques can reduce the distress attached to thoughts over time. Therapy tends to produce faster and more sustained results, particularly when thoughts have become persistent, are linked to compulsive responses, or are connected to past trauma.
Will Intrusive Thoughts Go Away?
Intrusive thoughts often become less frequent and less distressing when the brain no longer treats them as threats that require attention or control. Many people notice improvement once they understand how thought suppression, reassurance-seeking, and constant monitoring can unintentionally keep thoughts active. Evidence-based therapies such as CBT, ACT, and ERP help reduce the intensity and impact of intrusive thoughts over time. Even without therapy, learning how to respond differently to the thoughts can reduce how much space they take up.
Educational Disclaimer
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. If you're experiencing mental health concerns that interfere with your daily functioning, please reach out to a qualified mental health professional. If you're in crisis, contact your local crisis line or emergency services immediately.